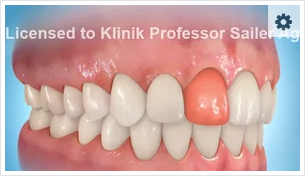
Tooth implants – the comfortable dental prosthesis solution after tooth loss
Implants are artificial tooth roots to which crowns and bridges are attached, but which also stabilise as removable dentures.
Ceramic implants are better
The Klinik Professor Sailer also offers, as well as titanium implants from leading manufacturers, the newest two-part ceramic implants made from zirconium dioxide. The latter have similar characteristics to titanium implants but also have a high degree of affinity to the gingiva and a low propensity to develop plaque. Ceramic implants fill a treatment gap which has existed for a long time. The crowns and bridges used are also manufactured from zirconium dioxide.
Professor Sailer was part of the developing team of the all-ceramic implant Zeramex. This is a completely metal-free implant. The material is particularly well-tolerated by the gingiva and mucous membranes, osseointegrates excellently with the jaw bones and, in the case of receding gums, cannot be differentiated from the ceramic dental prosthesis and is therefore hardly recognisable as an implant.
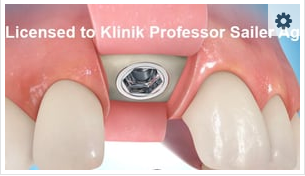
Course of treatment
The implants are inserted into the jaw bones. After a healing period of around 3-6 months, the bridges or crowns can be superimposed upon them. This can be either a single denture, a partial denture or a circular fixed denture in the case of a completely toothless jaw. The denture is manufactured according to functional and aesthetic considerations.
During the healing period of the implant, a temporary measure must usually be created. This can be an adhesive bridge or temporary partial prosthesis – completely independently of this, traditional clasp or model cast dentures have been consigned to history at the Klinik Professor Sailer. We provide our patients with bio-compatible materials which are also well-tolerated by patients with allergies.
Immediate implant
The demonstration video is only for illustrative purposes.
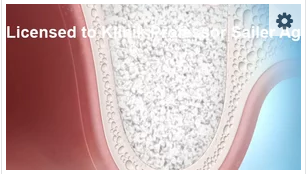
In cases of bone loss due to tooth removal or as a result of periodontal illness, bone augmentation is performed. The chin region or the zygomatic buttress serves as a point of removal of the bone. In case of large defects, the calvarium bone is taken. This technique has been developed at the Klinik Professor Sailer and used successfully for decades by Professor Sailer.

Illustration of the operation technique to insert an implant after filling the dental alveolus with bone substitute material.

Bone augmentation, jaw ridge enhancement
If minimal bone substance is available, the jaw bone must be augmented. We use different procedures to stimulate bone growth using the patient’s own bone, bone substitute materials and transpositional flaps. For a harmonious gum appearance, we replace tissue using transplantations and displacement procedures.
New dimensions in difficult implant situations – orthodontic surgery (Le Fort I) combined with bone transplants, sinus floor augmentation and the deployment of implants
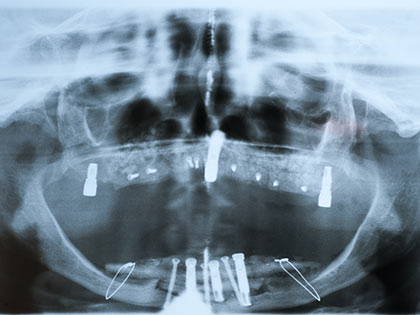
The OPT (fig. 3a) shows a serious shrinkage of upper and lower jaw bones (Cawood Class 6), the OPT (fig. 3b) shows the augmentation of the upper jaw with calvarium bone and a sinus inlay on both sides (calvarium bone).
Professor Sailer’s tripod method enables three implants with magnets (fig. 3b) to be inserted immediately, so that a temporary prosthesis can be worn in the upper jaw. At the same time, a complete ridge augmentation in the lower jaw with calvarium bone and the insertion of implants takes place, as a temporary measure. The OPT (fig 3c) shows the overall implant situation and the definitive prosthetic construction in the upper and lower jaw 3 years after the bone augmentation, without bone loss occurring. Zircon Implants (Zeramex®T) are the preferred implant system used today in the Klinik Professor Sailer.




Total reconstruction of the upper jaw plus Le Fort I with calvarium bone and immediate implantation (Professor Sailer’s tripod technique)
The patient was a female, 66 years old who had undergone numerous operations in other places with the aim of inserting implants:
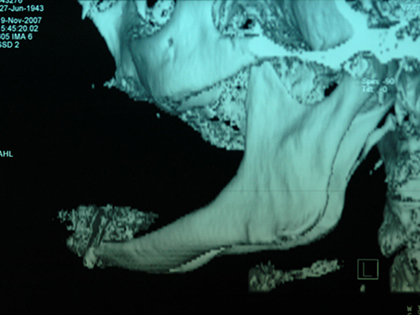
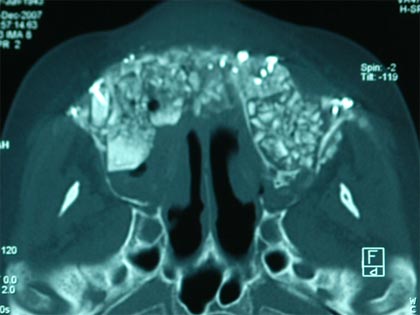
Sinus inlays, ridge augmentation with bones and implants all failed several times. The alveolar ridge is no longer there. Clearly visible in the OPT (Fig.1) and in the CT 3D reconstruction (Fig.2). Professor Sailer carried out a three dimensional reconstruction of the midface with the help of his special technique (Sailer, H.F.: A new method of inserting endossiours implants in totally atrophic maxillae. J.cranio-maxfac.surg.17 (1989) 299), where he uses cranial bones as transplant material visible in CT 3D. In the 3D computer tomograms in Fig.3, you can see the huge augmentation in the upper jaw area, consisting of calvarium bone and calvarium bone chips. Six months after this first operation, 12 implants were inserted into the reconstructed upper jaw, with four of them being furnished immediately with magnets, to fix a temporary prosthesis (Fig.4). After these operations, the appearance of the patient became normal and she looked many years younger.




Orthodontic surgery (Le Fort I) combined with bone transplants, sinus floor augmentation and the deployment of implants.
In this patient, 50 years old, (fig. 1), there was a growth disorder of the upper jaw, the basis of which lays too far back. At the same time the patient had lost the teeth in the upper jaw posterior region where, in addition, total ridge atrophy had occurred (fig. 2). Professor Sailer solved the problem using a combination of orthodontic and pre-prosthetic surgery by performing a Le Fort I osteotomy, moved the entire upper jaw forward into the optimal position for the lower jaw and, at the same time, removed the mucus from the maxillary sinus on both sides and filled these with calvarium bone. In the orthopantomogram (fig. 3), this first phase is represented. You can see an inserted temporary measure, so that the patient has teeth in the upper jaw, immediately after the operation. The orthopantomogram (fig. 4) shows the status six months later, after eight implants have been inserted in the upper jaw on both sides.





Sinus inlays in cases of bone loss
In cases of bone atrophy (bone loss), the jaw bone recedes as a result of tooth loss, meaning that implants cannot be anchored. Using a sinus inlay, bone material is embedded in the maxillary sinus, in order to be able to insert dental implants.
A sinus inlay is only possible, however, if there is healthy muscous membrane in the area to be operated on. If, instead of the muscous membrane, there is only scar tissue after a maxillary sinus operation or changes due to polyps or cysts following sinus infections, then a sinus inlay is not possible or is very risky, because blood supply to the tissue around the sinus inlay cannot be guaranteed. For the situations described, Professor Sailer has developed a technique which ensures the required blood supply for the inserted bones.
Illustration of the operation technique for a sinus inlay
The demonstration video is only for illustrative purposes.