These include congenital anomalies of the blood vessels (port-wine stains) and different forms of cancer of the skin and mucous membranes. Reconstructive surgery after tumours on the eyelids, lips and nose represent particular aesthetic and functional challenges. The preservation of the sensitive nervus trigeminus and the nervus facialis, needed for motoric and expressive function, take the highest priority.
Skin cancer of the face: Preservation of the nerves takes the highest priority
It is extremely important to take aesthetics, expressive function and the role of the face as our most important means of communication into account. This also applies in the case of tumour removals and defect reconstruction. The Klinik Professor Sailer has special nerve detectors which aid preparation in the facial area and reduce the risk of injuring the nerve to a minimum.
Body tattoos can also be removed
Using special surgical techniques, even extensive body tattoos which have been treated without success in the past can be removed. Professor Sailer is able to return exaggerated lips which have been over-injected to a beautiful shape and restore correct function.
Benign and cancerous changes of the exterior skin
Benign and cancerous skin changes (naevi, basal cell carcinomas, spinaliomas, melanomas etc.) are generally treated and removed by dermatologists. Large changes in various body regions and on the nose, at the corner of the eye, on the eyelids and lips, which lead to extensive resection defects, are treated using the operation techniques of reconstructive plastic surgery, which Prof. Sailer is using with highest expertise.
Patient report
Skin tumour removal on the nose
Mr. Delnon (see photos down below)
I had been observing a dark spot (lesion) on my left nostril for months: redness formed, then a crust, occasionally bleeding, and then it healed again.
I was worried that it was skin cancer (basalioma). I went to see Prof. Sailer, who had been the director of the Maxillofacial Surgery Clinic at the University Hospital Zurich for many years and operated on many tumours in the facial region. The sample biopsy confirmed my suspicions: it was malignant skin cancer (basalioma)!
Finally, surgical removal of the tumour was performed with the aid of multiple rapid incisions, and after microscopic confirmation of the absence of tumour in the adjacent tissues, immediate reconstruction of the approx. 2 cm roundish defect was performed.
I am extremely satisfied with the result. You can no longer tell that an operation had to be performed here.
Dr. med. dent Hans-Peter Delnon
Patient report
Mr. Karakurt, Switzerland
My story of misfortune and fortune that could only have been written by life itself!
About two years ago I developed extreme pain in the right cheek.
My dentist suspected an infected tooth root and thereupon began to treat each tooth in the right upper jaw, one after the other, without success and without discovering the cause of the pain. He prescribed me medication over and over again, which unfortunately did not help
My pain persisted and the many treatments took up a lot of time and posed an added burden to my already impaired health. I began to despair.
My dentist did not know what to do next and suspected I had a deeper infection. He therefore performed an operation in my mouth cavity to try, at long last, to get to the root of the problem. I felt very weak afterwards and had significant swelling. However the most devastating part of the whole procedure was that it was all for nothing – the pain was still there.
By then I was completely desperate, but my dentist reacted indignantly to this. I complained to him that he had treated me for half a year with no success at all. He appeared to have reached his limits and also had no idea what to do next. The only one chance I had left, he said, was to go to see the best specialists. And so he recommended Professor Sailer.
Professor Sailer is a completely different kind of doctor. A doctor that is interested in people, as is possible to see from the following lines.
Based on the previously unsuccessful results, he suspected a very serious diagnosis and sent a tissue sample for testing to an appropriate laboratory. The result was negative, meaning that everything was normal.
However, with his decades of experience, Professor Sailer found this hard to believe and sent a second tissue sample to a different laboratory. They again found nothing. Professor Sailer did not give up. He said that I was a young man with a family of three small children and the inconclusive search was unacceptable. “There has to be ‘something’ and we will find out what it is.” He thus sent a third tissue sample to a further laboratory, and we got back a result that should actually have been devastating to me: malignant cancer!
Nevertheless, my first reaction was relief at having finally discovered what was wrong with me. Professor Sailer immediately referred me to the most experienced oncologist to ensure I could get treatment as fast as possible. I was then given exactly the right chemotherapy for this type of cancer.
Today I now know that I had unbelievably good luck in my misfortune, because only a short time afterwards my body could have been full of metastasis, as this type of cancer is one of the family of blood cancers (leukaemia) that can spread very quickly throughout the entire body.
During the entire period of my chemotherapy treatment Professor Sailer and his colleague at the clinic, Dr. Jacobsen, rang me up again and again to check on my condition. No doctor had done this up to then.
Today, two years later, my health is very good again. I think of it as a nightmare from which I have finally awoken. It does not bear thinking about – that if I had never encountered this top medical expert and friend of the people, Professor Sailer, it could have ended differently and my children would no longer have a father.
I will never be able to express just how grateful I am to Professor Sailer.
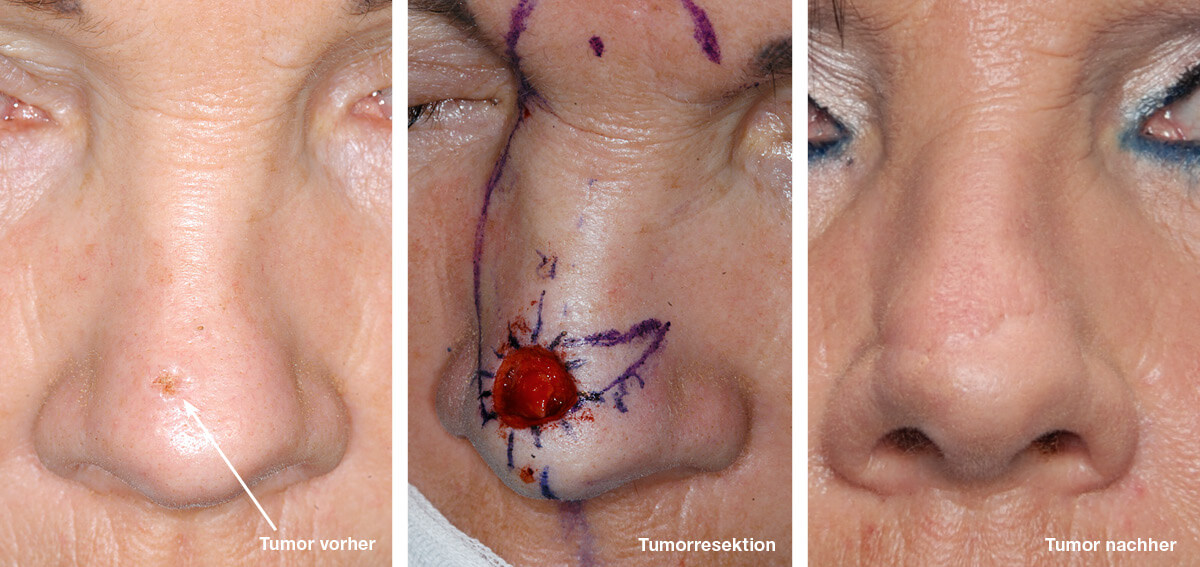
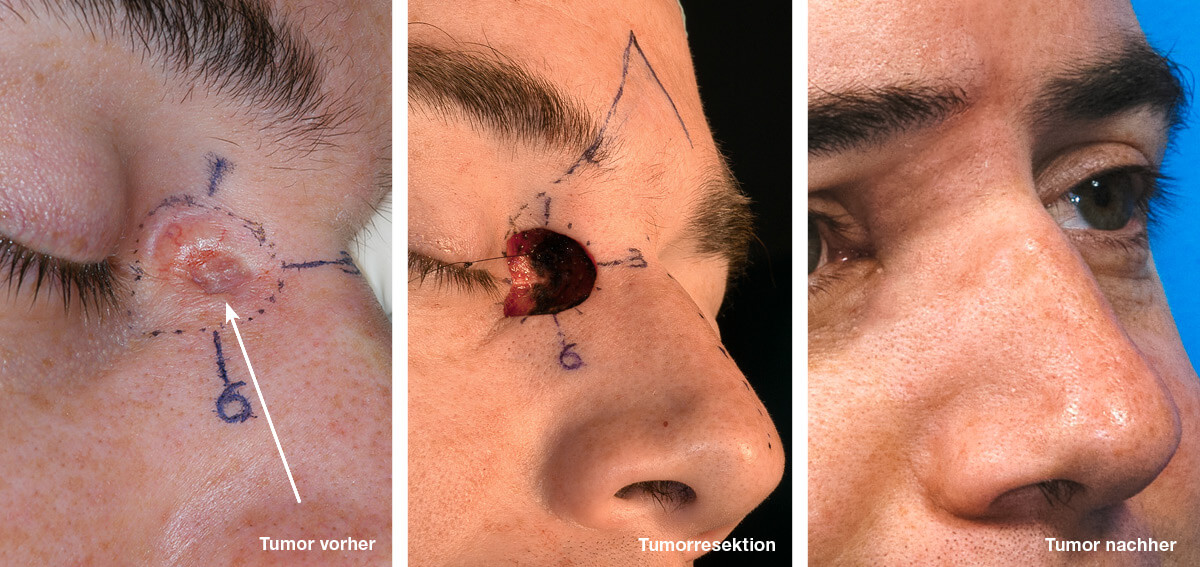
Case 1 skin cancer on nose
Photo on the left, before treatment: Skin cancer (basal cell carcinoma) on the bridge of the nose near the eye. Due to the malignant tumour, it is essential that surrounding tissue is also removed at the same time. In this case, at a diameter of 3cm.
Photo on the right, after the treatment: 10 months afterwards and the scars are hardly visible anymore.


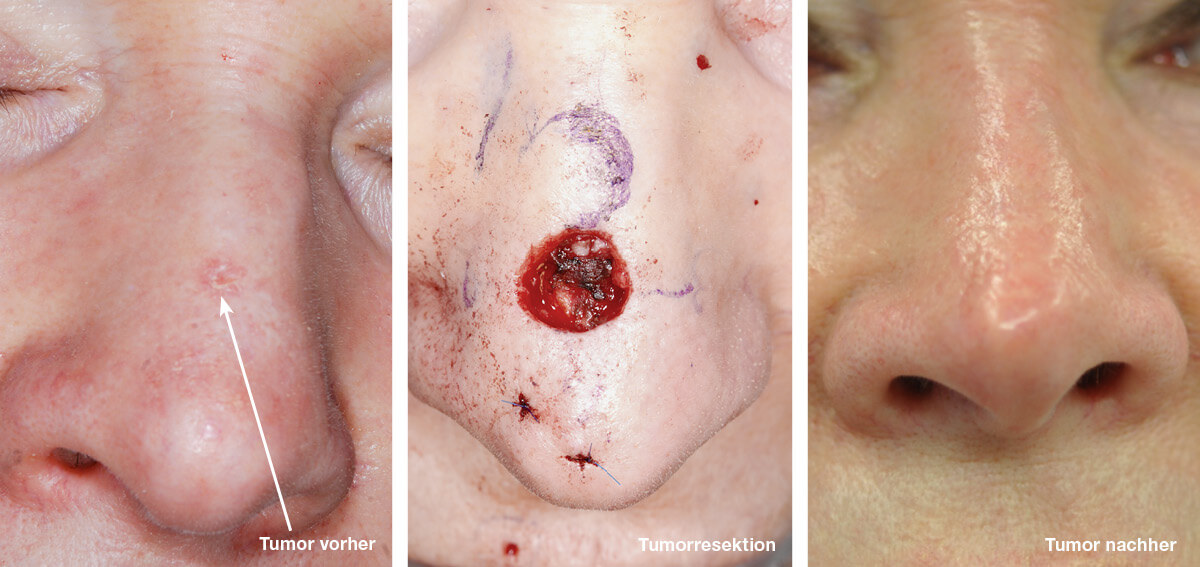
Case 2 skin cancer at the nose
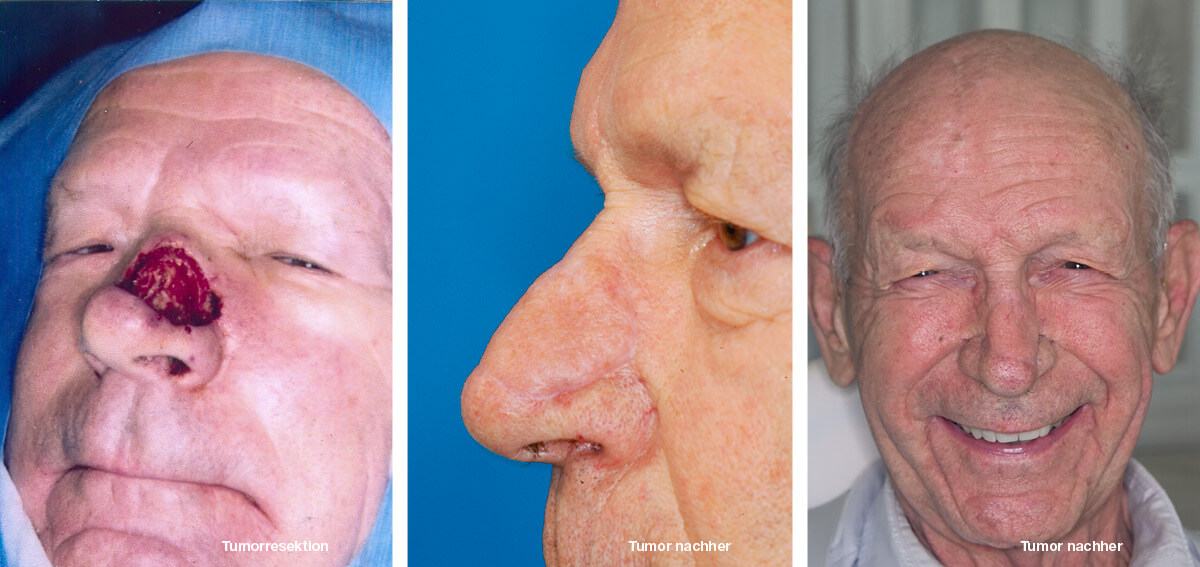
Photo on the left, before treatment: Enormous skin cancer (basal cell carcinoma) in the lower side nasal area. Due to the malignant tumour, it is essential that surrounding tissue is also removed at the same time.
Photo on the right, after the treatment: 6 weeks after defect coverage with glabella grafts and nasolabial grafts. Scars are hardly visible anymore.

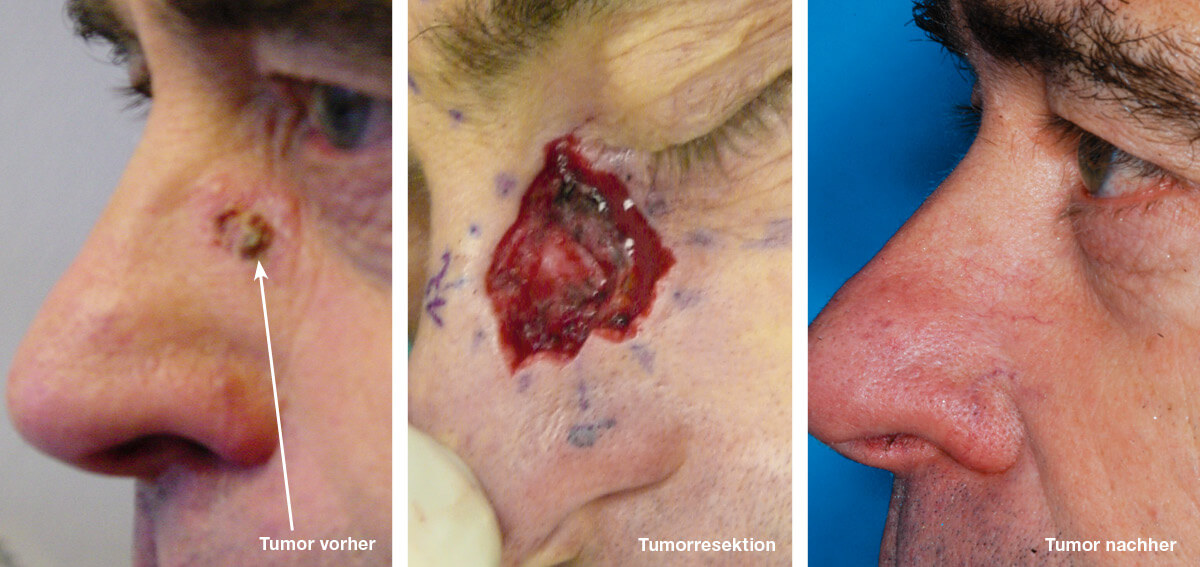
Case 3 skin cancer at the nasal ala
Left: Skin cancer (basal cell carcinoma) at the nasal ala. Due to the malignant tumor there must be removed surrounding tissue. In this case a diameter of 0,43 inches.
Right: Result without distortion of the nasal ala and without visible scars.


Case 4 skin cancer of the ear
Photo on the left, before treatment: Skin cancer (basal cell carcinoma) of the outer ear. Due to the malignant tumor, it is essential that surrounding tissue is also removed at the same time. In this case, at a diameter of 2.1cm.
Photo on the right, after the treatment: 6 months after reconstruction without deformation of the ear.



Before/after photos Mr Zuberbühler

Before/after photos Mr Delnon